Understanding the Nervous System Behind Weak or Painful Calves
When Your Calf Won’t Fire Properly
You might have heard a practitioner say something like:
“Your calf muscle is inhibited.”
For many people, that phrase can feel confusing.
Does it mean the muscle is weak?
Torn?
Or simply not working?
Recently, a patient asked this exact question online, and it sparked a deeper conversation about how the nervous system controls muscles.
The truth is surprisingly fascinating.
Often, when a calf muscle becomes “inhibited,” the problem is not the muscle itself — it’s the nervous system protecting the area.
Understanding this connection between pain, tendons, the spinal cord, and the brain can dramatically change how we approach recovery and rehabilitation.
At Neurohealth Wellness on Sydney’s Northern Beaches, we regularly see people with calf pain, Achilles issues, and lower limb dysfunction where the nervous system is playing a major role in limiting strength and movement.
Let’s unpack what’s really happening.
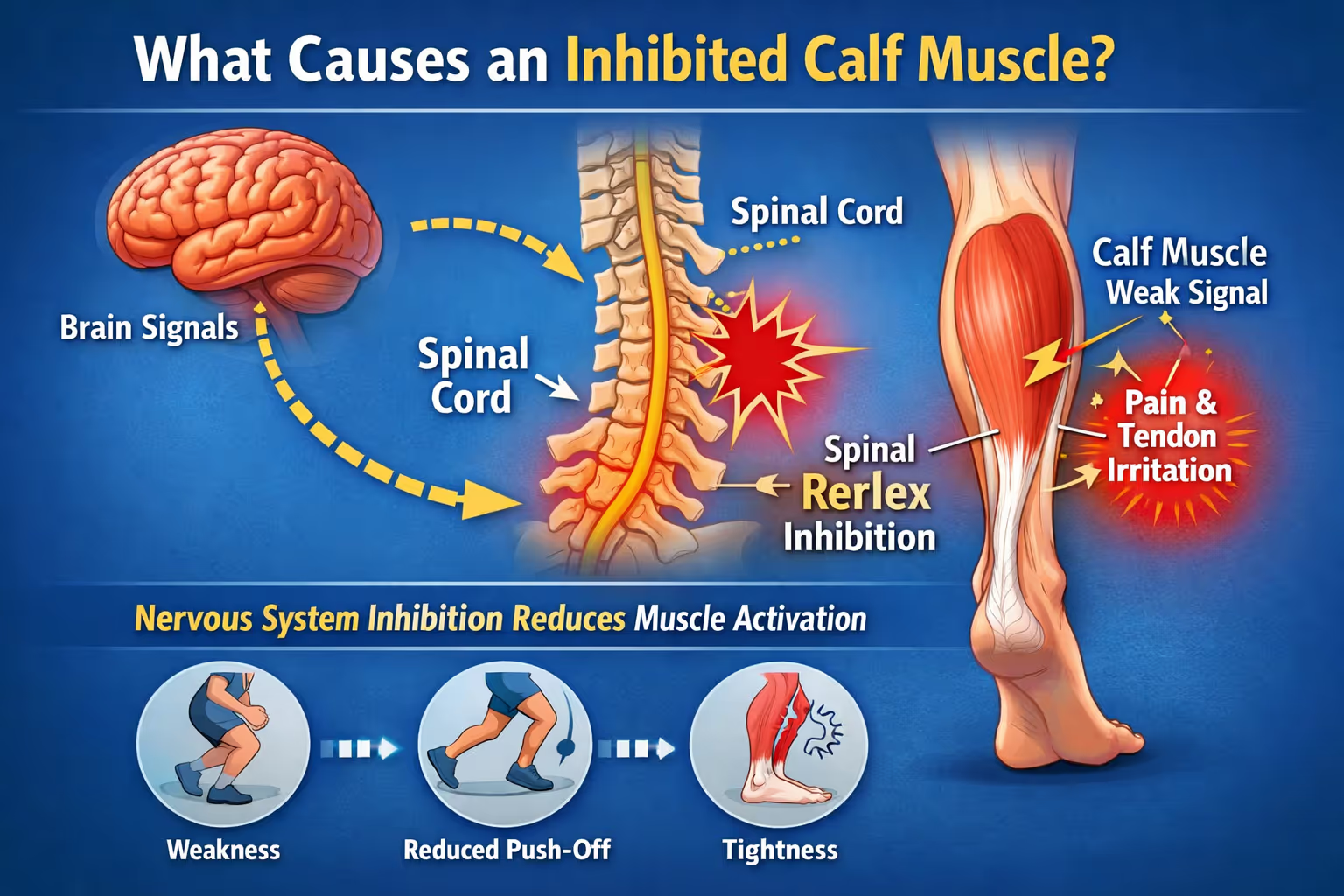
The Nervous System Controls Every Muscle You Move
Your muscles never work independently.
Every contraction happens because the brain sends electrical signals down the spinal cord and into the muscle.
If that signal is reduced, blocked, or inhibited, the muscle simply cannot generate its normal force.
Think of it like a dimmer switch.
The muscle might be structurally fine, but if the nervous system turns the dial down, the output drops.
This protective process is often called:
Arthrogenic Muscle Inhibition (AMI).
It’s the nervous system’s way of protecting an injured or irritated area.
Why a Calf Muscle Becomes “Inhibited”
There isn’t one single cause.
Inhibition can occur at three major levels:
- The tendon or muscle
- The spinal cord
- The brain
These levels constantly communicate with each other.
1. The Tendon and Local Reflexes
Most calf inhibition begins at the tendon level, especially with conditions like Achilles tendinopathy.
When a tendon becomes irritated or damaged, special sensory nerves called nociceptors detect the problem.
These receptors send signals to the spinal cord saying:
“Something isn’t right here.”
The spinal cord then activates inhibitory interneurons, which reduce the signal going back to the muscle.
The result?
The calf muscle cannot contract as strongly as it normally would.
This protective reflex reduces load on the injured tendon.
But there’s a catch.
Sometimes the nervous system becomes too protective, and the inhibition continues long after the tissue could tolerate load again.
2. Mechanical Sensors in the Muscle
Pain is not the only trigger.
The nervous system also monitors mechanical feedback from structures such as:
• Muscle spindles
• Golgi tendon organs
• Joint mechanoreceptors
If the information coming from these sensors becomes inconsistent — which can happen with tendon pathology — the nervous system may again reduce motor output as a protective strategy.
Essentially, the brain says:
“If I’m unsure what’s happening here, I’ll limit force just in case.”
This is why people with calf tendon injuries often report:
• Weak push-off
• Reduced jump strength
• Difficulty sprinting
• Persistent tightness
Even when the muscle itself appears normal.
3. The Brain’s Role in Muscle Inhibition
Beyond the spinal cord, the motor cortex in the brain also influences muscle activation.
Research has shown that people with tendon injuries often demonstrate increased cortical inhibition, meaning the brain reduces the signal sent to the muscle.
One well-known study examining athletes with patellar tendinopathy identified altered neural drive between the brain and the quadriceps muscle.
However, scientists still debate exactly where the main inhibition occurs.
In some cases, spinal inhibition dominates.
In others, the brain contributes more significantly.
Most likely, both systems interact together.
The Two Major Motor Pathways Most People Don’t Know About
A particularly interesting discovery in recent neuroscience research is that two different neural pathways control muscle force.
These are:
1. The Corticospinal Tract
This pathway specialises in precise, skilled movements.
It plays a dominant role in tasks such as:
• Fine hand movements
• Skill-based actions
• Coordinated exercise patterns
Rehabilitation exercises that involve rhythm, timing, or coordination tend to stimulate this pathway.
Examples include:
• Metronome-paced exercises
• Skill-based drills
• Controlled calf raises
2. The Reticulospinal Tract
This pathway is responsible for powerful, high-force movements.
It drives actions like:
• Sprinting
• Jumping
• Explosive strength
• Whole-body movements
Interestingly, emerging research suggests athletes with tendon pain may increase reticulospinal activity as a way to bypass inhibition and restore force production.
This system can help override spinal reflex inhibition.
Which is why rehabilitation often needs to include high-intent, powerful movements, not just slow controlled exercises.
Why Pain, Fear, and Confidence Matter
Another major factor influencing muscle inhibition is psychology and perception of safety.
Your brain constantly asks:
“Is this movement safe?”
If the answer is no, the nervous system may reduce motor output regardless of tissue health.
Fear of movement, pain catastrophising, and uncertainty can all increase neural inhibition.
This is why education and confidence building are such powerful tools in rehabilitation.
When someone understands what is happening in their body and begins moving successfully again, the brain often releases some of its protective inhibition.
How Do You Fix an Inhibited Calf?
Effective treatment usually requires a bottom-up and top-down approach.
In other words:
Address both the local tissues and the nervous system control mechanisms.
Step 1: Reduce Pain and Irritation
Pain strongly drives inhibition.
So the first priority is calming the irritated tendon or muscle.
This may involve:
• Load management
• Targeted strengthening
• Manual therapy
• Soft tissue work
• Dry needling or acupuncture
• Electrical stimulation such as TENS or EMS
At Neurohealth Wellness, our practitioners often combine chiropractic care, soft tissue therapy, cupping, and movement rehabilitation to reduce irritation and restore normal joint and muscle function.
👉 Ready to address persistent calf pain or weakness?
📍 Neurohealth Wellness – Northern Beaches, Sydney
📞 (02) 9905 9099
🌐 https://www.neurohealthwellness.com.au/booking
Step 2: Restore Normal Movement Signals
Once pain is settling, the next step is improving the mechanical signals travelling from the muscle back to the nervous system.
Exercises often start with:
• Slow calf raises
• Controlled loading
• Balance training
• Foot strengthening
These movements help normalise the sensory feedback that informs the nervous system about what the calf is doing.
This is one reason we often emphasise strong, resilient feet and ankle stability in our rehabilitation programs.
The foot is the foundation of the entire lower limb.
Step 3: Train Both Motor Pathways
A complete program should stimulate both neural pathways.
Corticospinal-focused training
Examples include:
• Metronome-paced calf raises
• Skill-based hopping drills
• Rhythm-based movements
These exercises improve coordination and motor control.
Reticulospinal-focused training
These exercises involve high intent and powerful effort, such as:
• Heavy calf raises
• Explosive jumping drills
• Sprint acceleration work
These movements encourage the nervous system to increase motor drive and overcome inhibition.
Both styles of training play a role in restoring full function.
The Most Important Factor: Feeling Safe to Move
Perhaps the most important ingredient in recovery is confidence in movement.
When the nervous system believes movement is safe:
• Motor output improves
• Protective inhibition reduces
• Strength returns faster
This is why rehabilitation should focus not just on exercises, but also on understanding the body and building confidence.
👉 Struggling with Achilles pain, calf tightness or recurring lower limb injuries?
Our team at Neurohealth Wellness focuses on restoring the nervous system control of movement, not just treating symptoms.
Book your assessment today.
📍 33–35 Kentwell Rd, Allambie Heights
📞 (02) 9905 9099
🌐 https://www.neurohealthwellness.com.au/booking
The Key Takeaway
An “inhibited calf muscle” does not simply mean weakness.
It usually reflects a complex interaction between:
• Tendon irritation
• Spinal reflexes
• Brain motor control
• Psychological safety signals
The muscle isn’t broken.
Often, the nervous system is simply trying to protect the body.
The goal of rehabilitation is to restore confidence, movement, and normal neural drive, allowing the calf to generate strength again.
Post Summary
An inhibited calf muscle occurs when the nervous system reduces the signal sent to the muscle, often due to tendon pain, spinal reflexes, or altered brain motor control. Effective rehabilitation addresses both local tissue irritation and nervous system motor pathways to restore strength and movement.
References
- Lepley AS, Lepley LK. Mechanisms of arthrogenic muscle inhibition. Journal of Sport Rehabilitation. 2021;31(6):707–716.
- Vallance P, Kidgell DJ, Malliaras P. Greater endogenous pain facilitation is associated with lower spinal excitability and maximal knee extension strength deficits in athletes with patellar tendinopathy. European Journal of Applied Physiology. 2026.
- Rio E, et al. Elevated corticospinal excitability in patellar tendinopathy compared with other anterior knee pain or no pain. Scandinavian Journal of Medicine & Science in Sports. 2016.
- Vallance P, et al. Transcranial magnetic stimulation and electrical stimulation techniques used to measure neuronal populations influencing motor output in musculoskeletal conditions. Journal of Electromyography and Kinesiology. 2025.
- Davi SM, et al. Quadriceps inhibition after naturally occurring patellar tendon damage and pain. Journal of Athletic Training. 2020.
- Akalu Y, et al. Identifying the role of the reticulospinal tract for strength and motor recovery. Physiological Reports. 2023.
- Vallance P, Malliaras P, Kidgell DJ. Cortico-reticulospinal excitability in athletes with patellar tendinopathy. Under review.
- Lecce E, et al. Resistance training-induced adaptations in the neuromuscular system. Journal of Physiology. 2026.
- Akalu Y, et al. Cortical and corticospinal responses to metronome-paced and self-paced strength training. European Journal of Applied Physiology. 2025.